Generic Medicines & the Rise of Jan Aushadhi Kendras in India: Promise, Pitfalls, and the Path Forward
A Movement in Progress
The expansion of generic medicines via Jan Aushadhi Kendras has been one of India's most significant public health interventions. With over 14,080 Kendras open by mid-2024—and growing—to replace patented medications with affordable, high-quality alternatives, the initiative aims to alleviate the burden of soaring out-of-pocket healthcare costs ippr.in+4x.com+4timesofindia.indiatimes.com+4timesofindia.indiatimes.com+5en.wikipedia.org+5en.wikipedia.org+5.
Yet it remains a contentious journey. On LinkedIn, senior healthcare leaders have voiced polarized views. While some celebrate it as a revolutionary step toward healthcare equity, others warn of regulatory gaps, quality concerns, and resistance from entrenched industry interests.
When journalist Durgesh Nandan Jha reported in Times of India recently, millions of Indian lives—and livelihoods—were reshaped by the generics revolution timesofindia.indiatimes.com.
Durgesh Nandan Jha’s Reporting: Numbers That Speak Volumes
In his June 27, 2025 article, “Why more Indians are ditching costly medicines — and trusting generics,” Jha shared illuminating stories and statistics:
- A diabetic-hypertensive couple, previously spending ~₹2,000/month, slashed their costs by 50–80% by switching to Jan Aushadhi generics x.com+1timesofindia.indiatimes.com+1timesofindia.indiatimes.com.
- Despite some doctors dismissing government generics as “low‐quality,” many users still trusted them when finances were tight muckrack.com+2x.com+2timesofindia.indiatimes.com+2.
These real-world examples underscore the economic lifeline Jan Aushadhi provides, particularly in vulnerable communities.
Global & Indian Context: Generics Are No New Concept
Generic medicines are globally accepted as safe alternatives to branded drugs once patents expire. In the US, generics make up over 90% of prescriptions, backed by strong bioequivalence and pharmacovigilance systems. India, post-1970 patents era, emerged as the “world’s pharmacy,” supplying roughly 20% of global generic demand and close to 40% of generics in the US ippr.in+5en.wikipedia.org+5academia.edu+5.
Yet, the Indian market’s growth has been uneven due to:
Brand-name distrust: With generics comprising only ~2–7% of prescriptions historically, public and prescriber trust has been slow to build .
Quality concerns: Counterfeit and substandard drugs, driven by regulatory lapses, have plagued the market en.wikipedia.org+3academia.edu+3timesofindia.indiatimes.com+3.
Profit-driven few: Studies show retail margins on generics can reach up to 1,000%, at times incentivizing irrational formulations over single-ingredient generic options ippr.in+1en.wikipedia.org+1.
Jan Aushadhi’s Reach & Economic Impact
The PMBJP (Jan Aushadhi) is not a small player—it’s a national initiative with a massive footprint:
- From 199 Kendras in 2008 to over 14,000 by mid‑2024, with ₹1,470 crore worth of generics sold in FY 2023–24 ippr.in+6en.wikipedia.org+6en.wikipedia.org+6.
- Over ₹30,000 crore saved since inception; ₹15,000 crore alone in fiscal 2024–25 .
- A diverse basket of 2,047 generic drugs and 300+ surgical products, including critical chronic disease medicines and even sanitary products .
Best-selling drugs include fixed-dose combinations like pantoprazole + domperidone (~1.08 million units/month), telmisartan (~930,000), and amlodipine (~850,000) timesofindia.indiatimes.com. These reflect chronic disease treatment—exactly the need underserved communities have.
Voices from LinkedIn: A Mixed Bag of Perspectives
🟢 Supportive Views
- Arindam Basu highlighted that accessibility and appropriate checks can coexist and not all generics are substandard.
- Dr. Shishir Patel pointed out the effectiveness of WHO‑GMP products through Jan Aushadhi and emphasized that high prices in branded drugs often arise not from quality but marketing.
🔴 Warnings & Caveats
- Dr. Manish Kondapuram urged caution: lack of bioequivalence testing, ADR tracking, and batch-wise accountability could lead to patient harm.
- Ambassador Mahendra Singh pushed back against big pharma designs, calling out cartel-like practices, even as he warned on quality lapses in government systems.
This dialogue reflects a deeper tension: affordability vs. assurance, with strong emotional and clinical stakes on both sides.
The Big Pharma Factor: The Other Uniform
Make no mistake—big pharma also has flaws. Branded drug costs are inflated by patent monopolies, aggressive marketing, and profit-driven FDC overuse. While generics are vilified, branded companies don’t always first advocate for patient affordability—yet they market trust in quality.
We need parallel accountability: not one-sided criticism of generics but scrutiny of all pharmaceutical players.
Pharmacovigilance: The Need of the Hour
To make Jan Aushadhi sustainable and trusted:
Mandatory Bioequivalence Testing
Every generic must prove therapeutic equivalence to its branded version before approval.
Batch Transparency via QR Codes
Linking packaging to manufacture data, lab results, expiry, and consumer feedback enhances traceability.
Cold-Chain & Storage Audits
For temperature-sensitive drugs (e.g., insulin, vaccines), systematic monitoring is vital.
Robust ADR Reporting Systems
Grassroots-level patient/clinician/mobile reporting must be integrated into a national pharmacovigilance network.
Third-Party Testing and Surprise Audits
Independent, NABL-accredited labs should routinely test samples from JAKs, with results published for accountability.
These are not idealistic asks—they are essential pillars to keep generics "low-cost, high-trust."
The Role of Doctors: Partners, Not Spectators
Physicians play a pivotal role. Based on LinkedIn comments:
- Instead of rejecting all generics, doctors should advocate for verified batches, educate patients, and document/report adverse events.
- In government facilities especially, prescribing generically rather than brand names—alongside transparency—can help reduce irrational prescribing driven by profit rather than evidence.
Reform Over Rejection
Jan Aushadhi Kendras symbolize what India’s healthcare can be: equitable, intentional, and scalable. But they are not yet infallible.
We must champion reforms, not condemnation:
- Enforce strict bioequivalence and TQM
- Implement real-time pharmacovigilance
- Make patient data and batch quality transparent
Let’s not sabotage this revolution over imperfections. Instead, let’s improve it—until affordable generics become synonymous with safe generics.
✅ Strengths⚠️ Risks🛠️ FixesMassive affordability & savings (₹30K+ cr)Bagged quality lapses, no transparencyBioequivalence tests, QR traceabilityReach: 14K+ KendrasCold-chain concerns, lack of ADR dataCold-chain audits, ADR systemsWHO-GMP sourcing, NABL testsIrregular and overt marketing pressureThird-party audits, prescriber accountability
Jan Aushadhi is not a panacea—it’s a platform. With pharmacovigilance, transparency, and collective responsibility, it can be the backbone of affordable, quality Indian healthcare.
#GenericMedicines #JanAushadhi #Pharmacovigilance #HealthcareEquity #DrugSafety #DurgeshNandanJha #PolicyReform #PublicHealthIndia
Related Articles
🏥 Hospital Boards Are Getting It Wrong If Your KPI is OPD Footfall, You’re Missing the Bigger Picture
Most hospital boards in Tier-2 India still track outdated metrics—OPD footfall, bed occupancy, and monthly billing—as signs of success. But in 2025, that’s no longer enough. Today, clinical outcomes, patient satisfaction, and operational efficiency matter more. Recent SME IPOs of small hospitals like Broach Lifecare and Shanmuga Hospital show that investors are backing value, not volume. Hospitals that shift from counting patients to improving care quality will lead the future of healthcare. Boards must evolve from revenue watchers to outcome enablers. Because in healthcare, impact matters more than intake.
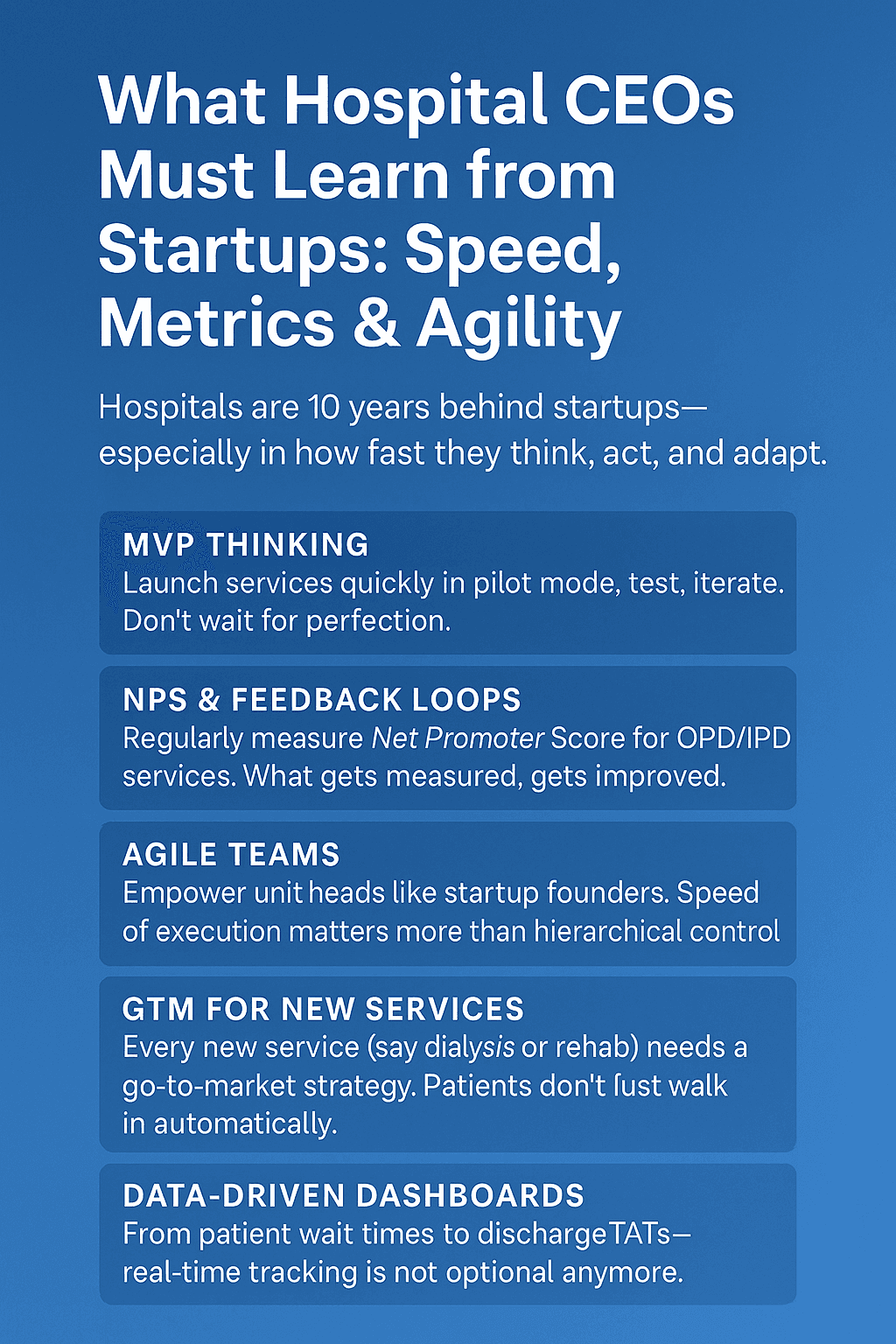
𝗪𝗵𝗮𝘁 𝗛𝗼𝘀𝗽𝗶𝘁𝗮𝗹 𝗖𝗘𝗢𝘀 𝗠𝘂𝘀𝘁 𝗟𝗲𝗮𝗿𝗻 𝗳𝗿𝗼𝗺 𝗦𝘁𝗮𝗿𝘁𝘂𝗽𝘀: 𝗦𝗽𝗲𝗲𝗱, 𝗠𝗲𝘁𝗿𝗶𝗰𝘀 & 𝗔𝗴𝗶𝗹𝗶𝘁𝘆
In today’s rapidly evolving healthcare landscape, traditional hospitals cannot afford to operate at yesterday’s pace. While startups are innovating at lightning speed—launching features, iterating on feedback, and scaling rapidly—many hospitals are still stuck in bureaucratic inertia, delayed decisions, and outdated management models. This article explores how hospital CEOs can adopt startup principles to drive operational efficiency, improve patient outcomes, and remain competitive. From MVP-based service launches to real-time dashboards, agile leadership structures, and data-driven decision-making, it outlines a practical roadmap for hospital leaders who are ready to embrace the mindset of a modern, patient-centric enterprise. The future of healthcare belongs to those who can move fast, measure right, and adapt with precision. It's time hospital leadership started thinking like entrepreneurs.

दिखावे के ज़माने में टूटते लोग: सोशल मीडिया, AI और हमारी अधूरी ज़िंदगी
सोशल मीडिया के इस तेज़ और चमकदार युग में, जहाँ हर मुस्कान में फिल्टर और हर रिश्ते में confusion है, वहाँ असली खुशी और सुकून दूर होता जा रहा है। हम सब दिखते बहुत 'happy' हैं, लेकिन अंदर से थके हुए, उलझे हुए और कभी-कभी टूटे हुए भी। AI से बात करना आसान हो गया है, पर अपने दिल की बात किसी अपने से कहना अब भी सबसे मुश्किल काम लगता है। ये लेख उसी नकली हँसी के पीछे छिपे दर्द, रिश्तों की उलझनों और mental health की सच्चाई को उजागर करता है – एक तंज, एक सच और एक कोशिश, कि शायद कोई पढ़कर रुक जाए... और खुद से या किसी से बात कर ले।
Syllabus ke bahar ka sawaal !
Busy in month-end closing? I bet you're deep in numbers: revenue, COGS, ROAS, margins, CAC, and all those financial metrics that keep the business world running. But let me ask you this: what about the numbers that truly matter? The numbers that can mean the difference between life and death?

Co-Working Spaces for Doctors: The New Age Revolution Beyond Polyclinics and Corporate Hospitals
India’s healthcare system is witnessing rapid transformation, and doctors, particularly those aiming to establish independent practices, face unprecedented challenges. The traditional polyclinic model, once seen as a practical solution for medical professionals looking to share resources and offer multi-specialty services under one roof, is now showing its limitations in a tech-driven world. Meanwhile, corporate hospitals and pharmacy-attached clinics are also proving restrictive for doctors, especially for those seeking autonomy, flexibility, and modern tools for patient care. Enter the era of co-working spaces for doctors, a dynamic business model that offers not only shared real estate but also a comprehensive tech-enabled ecosystem for doctors to thrive. From handling licensing and compliance to offering digital infrastructure for online appointments, telemedicine, CRM systems, and marketing solutions, these co-working spaces represent the next evolution in medical practice. In this article, we’ll explore the urgent need for such spaces in India, provide a detailed comparison between the old polyclinic model and new-age co-working spaces, and explain why this concept is better suited for doctors today—especially for specialists moving to suburban and smaller district towns.